Innovative telemedicine technology usage in rare diseases management in primary care in a COVID-19 pandemic era: Lessons learnt and recommendations for future practice
Adekunle Olowu
Consultant Family Physician, Primary Health Care Corporation, Doha, Qatar
Assistant Professor, Weill Cornell Medicine, Doha, Qatar
Clinical Assistant Professor, Qatar University College of Medicine, Doha, Qatar
Abstract
COVID-19 affected routine healthcare significantly and impaired the capability of healthcare organizations to deliver quality healthcare to achieve expected patient outcomes, including the care of patients with rare diseases. The rationale for this review is to highlight the important contribution of telemedicine technology to improving care quality of patients with rare diseases in a pandemic era.
Aims and Objective: To explore the role and impact of telemedicine digital technology usage and user satisfaction in patients with rare diseases in the last two years since the COVID-19 pandemic.
Methodology: An electronic database search was conducted using the PRISMA guide with search terms ‘telemedicine’ and ‘rare diseases’ in the last 2 years since the COVID-19 pandemic. The final search identified about 10 papers after screening, applying the exclusion criteria and sorting for eligibility and relevance.
Results: Of the 10 papers reviewed, 6 were research articles while 4 were review articles. For the research papers there were 5239 participants or responders in total, with 1476 (28.2%) patients, 50 (0.01%) carers and 3713 (70.9%) clinicians and workers. The average age recorded by 4 of the research papers was 43.4 years while one paper particularly emphasized that telemedicine digital technology was used preferably by clinicians below 50 years of age. 52.5% of Clinician and Worker participants in 2 Studies were Male while 47.5% were Female, while only 22% of patient participants were Male, with 78% being Female. One paper recorded the proportion of patients who used telemedicine as 22.8 %, a second recorded the highest proportion of clinicians’ telemedicine usage as 59.8%, a third paper concluded the highest number of carers who were satisfied with telemedicine usage was 90%, with 58% also supporting its usage and a fourth recorded that 86% of patients were satisfied with its usage. However, another paper recorded that 26% of clinicians (psychiatrists) were not keen to use telemedicine.
Conclusion: This review concludes that there is some evidence that telemedicine digital technology is a viable option and can be a long-term solution to primary care patients’ access to quality care in the post-pandemic era, including patients with rare diseases. International collaboration of clinicians via electronic or digital platforms will enhance quality of care, especially targeted to younger male physicians below the age of 50. Guidelines and protocol for its use within governmental laws and legal boundaries need to be strictly followed to ensure patient safety, reduce waiting times and achieve positive patient outcomes.
Introduction
The COVID-19 Virus caused by severe acute respiratory syndrome Coronavirus (SARS-COV2) outbreak started in Wuhan, China in December 2019 when pneumonia was diagnosed in several patients. It was later declared a pandemic by WHO few months later and has led to significant morbidity and mortality globally1. According to the WHO, as of 30th July 2022, there had been 567 million confirmed cases and 6.3 million deaths globally2. The COVID-19 pandemic impaired the capability of healthcare organizations and providers globally to deliver quality healthcare services to achieve expected key performance indicators and positive patient outcomes. It has also significantly impacted the routine healthcare of patients with rare diseases, especially their access to services and relevant medication3,4. However, the pandemic provided many opportunities for innovative technological applications to improve patient flow and access to care, some of which will be reviewed in this paper5,6. Ongoing and future research on technological applications to achieve patient safety will provide further evidence on guidelines and protocol in telemedicine applications, but the author explores what the options are in current literature and their impact on the care of patients with rare diseases7,8,9,14. This aim of this review is to highlight the challenges faced by rare diseases patients and their carers during the COVID-19 pandemic through a literature review of ten papers, as well as emphasize the crucial role digital telemedicine technology plays in improving the quality of care of patients with rare diseases in a pandemic era. ‘Digital telemedicine technology’ in this discourse refers largely to telephone consultations.
Methodology
Sources like PubMed, Clinical Key, Access Medicine, Google scholar, Web of Science, ProQuest Research Library, ScienceDirect, DynaMed, UpToDate, SciVal, and Brow Zine were searched via an online library platform. The PRISMA guide was utilized for identification, screening, eligibility, and inclusion of studies in this review. Search terms used include ‘telemedicine’ and ‘rare diseases.’ The exclusion criteria included secondary or community care papers, obstetrics & gynecology papers, online-based surveys, management of relatively common conditions, purely laboratory studies, purely genetic studies, some rare case reports and chronic or long-term conditions. Included articles were online access full-text, human, peer-reviewed articles in English published in the last 2 years. The study was limited to 2 years to restrict the scope and include most recent papers since the onset of the COVID-19 pandemic. The final search identified 10 relevant studies after screening, applying the exclusion criteria and sorting for eligibility and relevance, 4 of which were review articles. Participants or responders to surveys or questionnaires in all the studies were analysed and the results were presented10,11. [Figure 1]
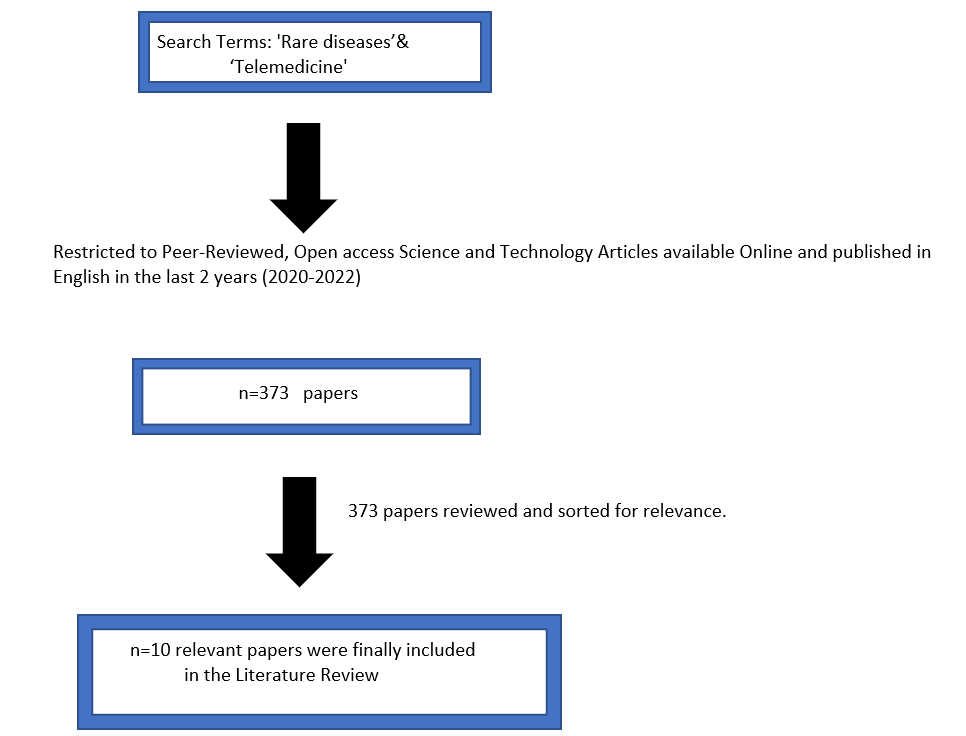
Figure 1: PRISMA Paper selection
Results
Of the ten papers reviewed, six were research papers while four were review articles. For the reviewed papers there were 5239 participants in total, with 1476 (28.2%) patients, 50 (0.01%) carers and 3713 (70.9%) clinicians and workers (5239 was from a simple addition of all the respondents or participants in the research papers reviewed) [Figures 2a, 2b & Table 2]. The average age recorded by four of the research papers were 43.4 years, while one paper particularly emphasized telemedicine digital technology which clinicians particularly preferably used below 50 years of age. 52.5% of Clinician and Worker participants in two studies were Male while 47.5% were Female, while only 22% of patient participants were Male, with 78% being Female. [Figure 3 & Tables 3a and 3b] One paper recorded the proportion of patients who used telemedicine as 22.8 %, a second recorded the highest proportion of clinicians’ telemedicine usage as 59.8%, a third paper concluded the highest number of carers who were satisfied with telemedicine usage was 90%, with 58% also supporting its usage and a fourth recorded that 86% of patients were satisfied with its usage [Figure 4]. However, another paper recorded that 26% of clinicians (psychiatrists) were not keen to use telemedicine. [Figure 4 & Table 4] Qualitative statistical analysis was not done.
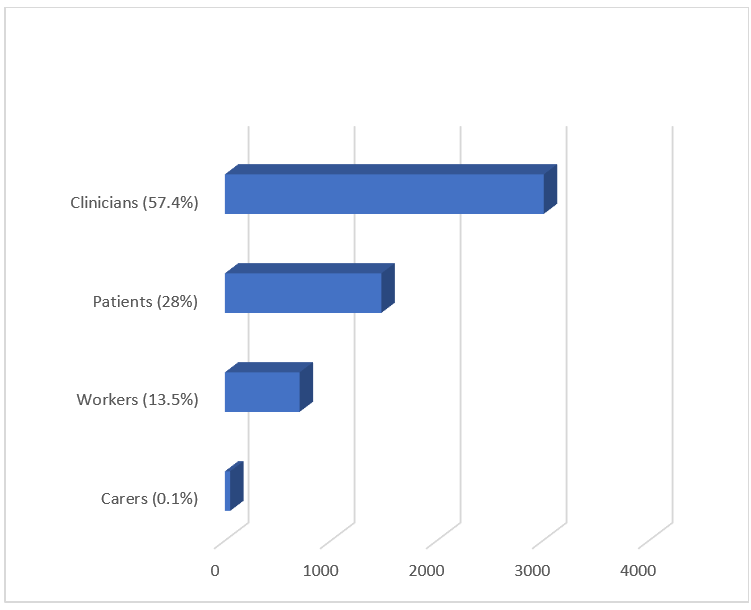
Figure 2a: Proportion of Study Participants
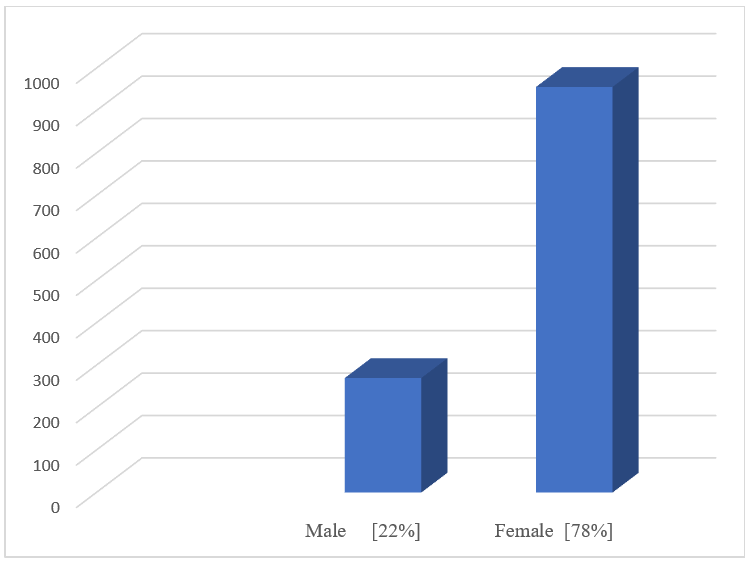
Figure 2b: Sex of Patient Participants
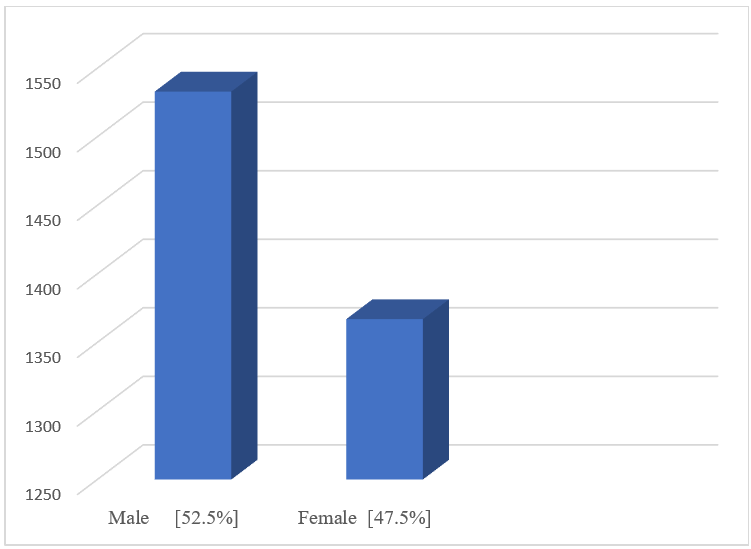
Figure 3: Sex of Clinic. Participants
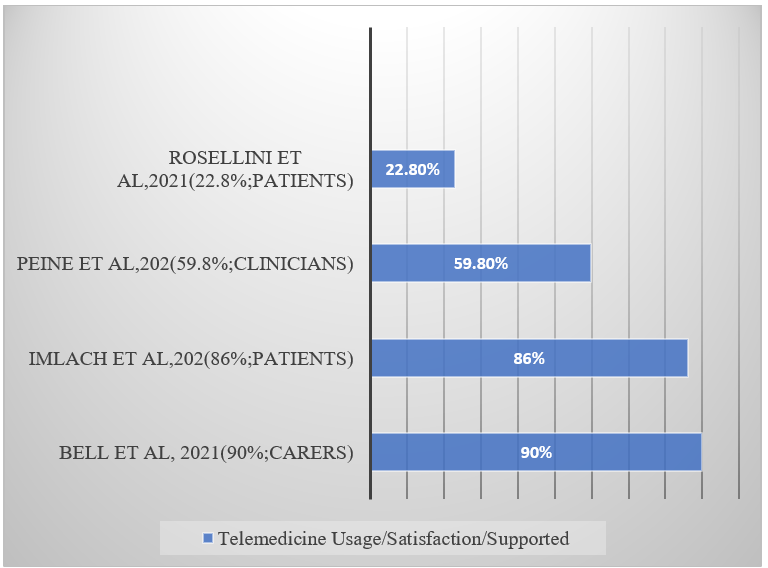
Figure 4: Telemedicine Usage/satisfaction/Supported.
Table 1: Characteristics of papers included in the literature review.
|
Author/Yr. of Publication/ Country |
Study Population |
No. of Participants or Respondents |
Study design |
Av. Age (yrs.) |
Sex (%) |
Participant Satisfaction |
Telemedicine Technology Usage |
Telemedicine Technology Supported |
Telemedicine Technology Unsupported |
|
Bell et al. 2021 (UK) |
Genetic Diseases Patients and Carers |
50 |
Questionnaire Survey |
N/A |
N/A |
90% |
Yes |
Yes (58%) |
No |
|
Chowdhury et al. 2020 (USA) |
Pediatric Cardiology practitioners |
N/A |
Review Article |
N/A |
N/A |
N/A |
Yes |
Yes |
No |
|
Duffy et al. 2016 (USA) |
Psychiatrists |
152 |
Systematic review |
39 yrs. |
M (58%)/F (42%) |
N/A |
Yes |
Yes |
26% |
|
Halderman et al. 2021 (International) |
Clinicians |
29 |
Review |
N/A |
N/A |
N/A |
Yes |
Yes |
No |
|
Imlach et al. 2020 (New Zealand) |
Patients |
1048 |
Online Survey & Interviews |
N/A |
M (84.5%)/F (14.2%) |
86% |
Yes |
Yes |
No |
|
Naveen et al. 2021 (India) |
Patients |
250 |
Prospective Study |
38 yrs. |
N/A |
N/A |
Yes |
Yes |
No |
|
Nitiema. 2020 (International) |
Health Care Workers |
705 |
Online Survey |
N/A |
N/A |
N/A |
Yes |
Yes |
No |
|
Peine et al. 2020 (Germany) |
Clinicians |
2827 |
Online Survey |
43 yrs. |
M (51.1%)/ F (46.1%) |
N/A |
Yes (59.8%) |
Yes |
No |
|
Rosellini et al. 2021 (Italy) |
Chronic Neuro. Patients |
178 |
Observational Study |
53.5 yrs. |
M (39%)/F (61%) |
N/A |
Yes (22.8%) |
Yes |
No |
|
Spina et al. 2021 (Italy) |
Patients |
N/A |
Review article |
N/A |
N/A |
N/A |
Yes |
Yes |
No |
|
Totals |
|
5239 |
|
|
|
|
|
|
|
Table 2: Proportion of Study Participants/Responders.
|
Carers (0.1%) |
50 |
|
Workers (13.5%) |
705 |
|
Patients (28%) |
1476 |
|
Clinicians& Workers (57.4%) |
3008 |
|
Total (100%) |
5239 |
Table 3a: Sex of Clinician Participants/Responders.
|
Male [52.5%] |
1533 |
|
Female [47.5%] |
1367 |
|
Total [100%] |
2900 |
Table 3b: Sex of Patient Participants/Responders.
|
Male [22%] |
270 |
|
Female [78%] |
956 |
|
Total [100%] |
1226 |
Table 4: Telemedicine Usage/Satisfaction/Supported.
|
Bell et al. 2021 (90%; carers) |
90% |
|
Imlach et al. 2020 (86%; patients) |
86% |
|
Peine et al. 2020 (59.8%; clinicians) |
59.80% |
|
Rosellini et al. 2021 (22.8%; patients) |
22.80% |
Discussion
Digital technological applications in healthcare vary from the use of computer devices with patient’s electronic medical records (EMR) and smart phones with mobile apps to more specialized software usage, usage of thermal image scanning, telehealth, electronic patient check-in systems and home testing kits, as well as personalized genomic medicine. More complex devices like the Radio-frequency identification (RFID) and Infrared (IR) systems used for patient tracking have also been used, according to a paper exploring electronic patient tracking through an ambulatory clinic, though their digital technology was expensive which may hinder its wider application11. Another study by Martinego et al. (2020) highlighted the crucial additional role that mobile phone messaging plays in professional patient communication for reminding them about appointments, repeat prescriptions, medications adherence, sharing of information, laboratory results, management of long-term conditions and health promotion14. With the advent of the COVID-19 pandemic, it is pertinent to highlight the role digital health technology played in the management of infectious diseases e.g., SARS, H1N1, Ebola viruses and the COVID-19 coronavirus as revealed in a recently published paper. It clearly identified the importance of prioritizing prevention of spread to health care providers considered as high-risk groups and used digital triage, digital diagnosis, monitoring and contact tracing. However, the paper was limited to digital health application in infectious diseases transmission prevention only15,17. This review highlights the key role that telephone consultations utilization in the management of patients with rare diseases plays, use of telemedicine digital technology in caring for patients has a varied uptake by physicians globally, and its successful application to achieve positive outcomes for primary care patients depend on buy-in by patients, carers, and primary care providers. A random American survey of 152 psychiatrists showed that though majority of them were comfortable using computers for personal and educational purposes, 26% reported they were not comfortable using it for clinical purposes, especially those above 50 years old7. [Table 1] Another study exploring the experiences and preferences of patients about telehealth consultations concluded that they reported high levels of satisfaction, though the survey was short as it was conducted during a pandemic lockdown and there were problems with communication, costs, and privacy issues that needed to be resolved3.
Napoles et al. (2016) explored staff perceptions about digital technology and concluded that staffing levels, availability of resources and training were facilitating factors while visit time constraints and patients’ complex healthcare needs were hindering factors16. An International study reviewing health care providers’ opinions about telehealth uptake post pandemic concluded that their opinions about telehealth benefits were less positive during the pandemic compared to the pre-pandemic period. They also observed some challenges during the pandemic including technical problems encountered during telehealth sessions and the inability to perform certain care routines through telehealth platforms, as well as potential legal and financial challenges4.
In addition, a multi-country study on innovative remote diagnosis and monitoring during the COVID-19 pandemic concluded that telemonitoring using several devices including video cameras especially in times of crisis has come to stay, but privacy and ethical issues may need to be resolved17. One of the other challenges identified in some of these studies was that the needs of patients with rare diseases varied with their clinical condition and that there would be a need to adapt telemedicine technological devices to their needs, as well as to the needs of their carers. While the COVID-19 pandemic caused significant havoc for health systems globally, leaders and managers of health institutions explored novel approaches to improving access and quality of care for patients. Rare diseases sufferers were particularly disadvantaged as some aspects of their care were already deficient, which the pandemic only worsened, with disruptions and increased footfall leading to patient delays, difficulties in accessing routine care and challenges with obtaining appropriate medication5,15. Telemedicine consultations were rapidly introduced into routine healthcare by providers in most healthcare organizations to help improve patient access. For example, the author's primary health care organization (which manages rare disease patients amongst others) recorded an increase in the proportion of telephone consultations from none (0%) in 2019 (pre-COVID-19 pandemic) to 26% in 2020 (during the COVID-19 pandemic). 18% of all telephone consultations in 2021 were with patients with high-risk conditions18. A New Zealand study exploring telehealth use during the pandemic revealed high patient satisfaction, and that it was very convenient and effective for routine cases, and less useful when a physical examination was required or when the diagnosis was unknown3.
These findings were like those in the literature review. According to a German study, 39% of clinical staff responders rated the significance of telemedicine as high, and that telemedicine was already in routine or partial use by 59.8% of healthcare providers19. [Table 1; Figure 4] A genetic eye diseases study concluded that 58% of participants found teleconsultations acceptable and 54% agreed they increased their access to care, but 67.5% preferred to be seen in person, while patient satisfaction was high at 90%25. [Table 1; Figure 4] Virtual visits via the use of Google Meet was another modality employed during COVID-19 for the care of chronic neurological patients, according to Rosellini et al. (2021) who demonstrated their feasibility and efficacy20. In their study, Naveen et al. (2021) discovered that voice-based teleconsultations may be useful to diagnose and manage relapses in Idiopathic Inflammatory Myopathies21. Yet another one recommended the use of remote-controlled apps by clinicians in engaging neuromuscular diseases patients22. However, for telehealth to be effective for patient care without causing significant potential medico-legal and financial complications, there needs to be appropriate guidelines developed to guide healthcare practitioners in their safe usage, as was done by Abbott et al. (2020) who conducted a review of literature supporting the development of practice guidelines for tele-dermatology in Australia. The guideline document educates providers about the benefits and limitations of telehealth while articulating how to enhance patient care and reduce risk when practicing tele-dermatology9. Another study on remote management of spinal patients concluded that guides are valuable during times of government-mandated social distancing due to infectious diseases like the COVID-19 pandemic, and that these guides should be helpful in underserved communities in several countries where there is a shortage of accessible trained spine care clinicians. They have the potential of reducing overutilization of unnecessary and expensive interventions while empowering patients to manage uncomplicated spinal pain themselves assisted by their clinician, either through direct in-person consultation or via telehealth communication23. The WHO has also prepared a useful guideline and plan for using telemedicine in children and adolescents24. International telemedicine diagnostic initiatives need to be encouraged, as highlighted by a Dominican Republic study exploring improving access to genetic services which concluded there was evidence to support an international telemedicine diagnostic service linking pediatricians and geneticists26,27. Also, telemedicine sustainability explored by Chowdhury et al. in their American paper on the use of telehealth in pediatric cardiology, concluded that sustainability of the online method of pediatric cardiology service delivery will require tweaking of tele-healthcare strategies, defining best practices, telehealth inclusion in the postgraduate medical fellowship curriculum and continuing advocacy for technology. However, technology is not without its drawbacks. It can be expensive and non-homogenous, with lack of infrastructure and limited access to patients in some countries. It can also be perceived by some patients as impersonal and fraught with privacy and confidentiality issues12,26,27,28. Despite these drawbacks, to improve patient flow and access to care of primary care patients including rare disease patients, other novel innovative devices like the Electronic Patient Communications and Information Leaflets system (EPCILs) should be explored, as proposed by the author in a dissertation as a quality improvement initiative. It aims to achieve waiting time reduction by 50% so 85% of patients are seen within 30 minutes, improve patient experience rating to 50% and improve the ‘excellent’ patient safety rating to 50% within 6 months of its application. It is a planned project which also aims to provide health awareness, health prevention and streamline patient flow within the country’s health centers. EPCILs aims to apply the 2018 HSE Model for change, utilizing Lean’s ideology, with evaluation of planned results to be achieved via EMR data, PDSA, the ‘Before-and-After’ Study and Staff and Patients questionnaire survey29,30,31,32,33,34,35. Hopefully, this will achieve better patient satisfaction, improve patient experience, attain patient safety and increase organizational efficiency. Williamson (2016) emphasized the importance of electronic check-in systems in primary care while Howe and Geraldi (2012) highlighted how the Gantt chart helps manage the project timeline, with its cost projections, risks, and benefits noted27,31,32,33,34,39. However, quality improvement projects for positive healthcare outcomes must be affordable and cost effective. Saha et al. (2013)’s analytical study on the cost-effectiveness and QALY (Quality Adjusted Life Year) of lifestyle interventions in primary care found that though costs were projected to increase both short-term and long-term, there was an average cost reduction of $700 in the short-term and $7,300, compared with intervention cost of $211 participant, resulting in cost savings. For EPCILs, the author assessed its cost-effectiveness through a budget impact analysis which revealed that it was affordable36,37,38. Electronic patient access systems are becoming popular worldwide, though uptake is still generally low, according to Bush et al. (2019) whose paper exploring pediatric urology patient portal access activation concluded that only 19.3% of the 48.9% of patients granted access codes activated it13. [Table 1]
Conclusion
This review was conducted to emphasize some evidence on the role digital technology and telemedicine played in improving the pandemic management of patients in primary care, including rare disease patients. It is especially relevant for male clinicians below the age of fifty but is applicable to all clinicians as well as patients and their careers. It enables improved access to services and essential medication, reduces patient waiting time for appointments and significantly helps in routine care and follow up3,4,10,29. However, digital technologies and telemedicine have potential regulatory and legal challenges that need to be surmounted to provide services that lead to sustainable patient outcomes. This requires effective healthcare leadership and national and international collaboration between health care providers globally to develop and apply evidence-based guidelines on the use of digital technologies including telemedicine to implement it effectively and efficiently, especially tailored to the needs of rare diseases patients7,9,17,23,41. Though the literature review highlighted in this review was on a small number of papers, future well-designed prospective research will be needed to further assess telemedicine utilization on a wider scale and over several years post-COVID-19 pandemic in rare diseases patients, with a comparative analysis of both patients’ and clinicians’ experiences.
Funding
The author declares that no funding was obtained for this paper as at the point of publication, but the author is grateful to Qatar National Library for their support.
Conflict of Interest
The author declares that there are no conflicts of interest regarding this paper.
Ethical Approval or Consent for publication
The author declares that this paper does not need any ethical approval or consent for publication.
References
- World Health Organization (2020) Novel coronavirus (2019-nCOV) situation reports. https://biy.ly/2UVXVsD. Accessed 30 July 2020. Coronavirus Disease (COVID-19) Situation Reports (who.int).
- World Health Organization (2022) Weekly epidemiological update on COVID-19 - 27 July 2022 (who.int).
- Imlach F, McKinlay E, Middleton L, et al. Telehealth consultation in general practice during a pandemic lockdown: survey and interviews on patient experiences and preferences. BMC Family Practice. 2020; 21: 269. https://doi.org/10.1186/s12875-020-01336-1
- Nitiema P. Telehealth Before and During the COVID-19 Pandemic: Analysis of Health Care Workers' Opinions. Journal of Medical Internet Research. 2022; 24(2): e29519. https://doi.org/10.2196/29519
- Calton B, Abedini N, Fratkin M. Telemedicine in the Time of Coronavirus. Journal of Pain and Symptom Management. 2020; 60(1): 8.
- Hollander JE, Carr BG. Virtually Perfect? Telemedicine for Covid-19 New England Journal of Medicine. 2020; 382: 18.
- Duffy FF, Fochtmann LJ, Clarke DE, et al. Psychiatrists’ Comfort Using Computers and Other Electronic Devices in Clinical Practice. Psychiatry Q. 2016; 87(3): 571-584.
- Gulhan I. A unique e-health and telemedicine implementation: European Reference Networks for rare diseases. Journal of Public Health: From Theory to Practice. 2020; 28: 223-225. https://doi.org/10.1007/s10389-019-01052-w
- Abbott LM, Miller R, Janda M, et al. A review of literature supporting the development of practice guidelines for tele dermatology in Australia. Australasian Journal of Dermatology. 2020; 61: e174-e183.
- Bates DW, Gawande AA. Improving patient safety with information technology. New England Journal of Medicine. 2003; 348: 2526-34. Available at https://www.qatar-weill.cornell.edu/library
- PRISMA Statement. Available at https://prisma-statement.org//
- Vakili S, Pandit R, Singman EL, et al. A comparison of commercial and custom-made electronic tracking systems to measure patient flow through an ambulatory clinic. International Journal of Health Geographics. 2015; 14: 32.
- Bush RA, Vemulakonda VM, Richardson AC, et al. Providing Access: Differences in Pediatric Portal Activation Begin at Patient Check-in. Appl Clinical Information. 2019, 10(4): 670-678.
- Martinego L, Spinazze P, Car J. Mobile messaging with patients. BMJ. 2020.
- Alwashmi MF. The Use of Digital Health in the Detection and Management of COVID-19. International Journal of Environmental Research and Public Health. 2020; 17: 2906.
- Napoles AN, Appelle N, Kalkhoran S, et al. Perceptions of clinicians and staff about the use of digital technology in primary care: qualitative interviews prior to implementation of a computer-facilitated 5As intervention. BMC Medical Informatics and Decision Making. 2016; 16: 44.
- Behar JA, Liu C, Kotzen K, et al. Remote health Diagnosis and monitoring in the time of COVID-19. Physiological Measurement. 2020.
- PHCC Corporate Annual Statistical Report. 2021.
- Peine A, Paffenholz P, Martin L, et al. Telemedicine in Germany During the COVID-19 Pandemic: Multi-Professional National Survey. Journal of Medical Internet Research. 2020. Available at https://www.jmir.org/2020/8/e19745
- Rosellini I, Vianello M, Ghazaryan A, et al. Virtual Visits for Chronic Neurologic Disorders during COVID-19 Pandemic. Neurological Sciences. 2021; 42: 2607-2610. https://doi.org/10.1007/s10072-021-05212-3
- Naveen R, Sundaram TG, Agarwal V, et al. Teleconsultation experience with the idiopathic inflammatory myopathies: a prospective observational cohort study during the COVID-19 pandemic. Rheumatology International. 2021; 41: 67-76.
- Spina E, Trojsi F, Tozza S, et.al. How to manage with telemedicine people with neuromuscular diseases? Neurological Sciences. 2021; 42: 3553-3559. https://doi.org/10.1007/s10072-021-05396-8
- Halderman S, Nordin M, Tavares P, et al. Distance management of Spinal Disorders During the COVID-19 Pandemic and Beyond: Evidence-based patient and clinician guides from the Global Spine care Initiative. JMIR Public health Surveillance. 2021; 7(2): e25484.
- WHO (2021). How to plan and conduct telehealth consultations with children and adolescents and their families Geneva: World health Organization; 2021. Licence: CC BY-NC-SA 3.0 IGO.
- Bell S, Karamchandani U, Malcolmson K, et al. Acceptability of Tele genetics for Families with Genetic Eye Diseases. Genes. 2021. Available at https://doi.org/10.3390/genes12020276
- Mena R, Mendoza E, Pena MG, et al. An international telemedicine program for diagnosis of genetic disorders: Partnership of pediatrician and geneticist. Am J Med Genet C Semin Med Genet. 2020; 184(4): 996-1008.
- Chowdhury D, Hope KD, Arthur LC, et al. Telehealth for Paediatric cardiology Practitioners in the Time of COVID-19. Paediatric Cardiology. 2020; 41: 1081-1091. https://doi.org/10.1007/s00246-020-02411-1
- Williamson C. Electronic self check-in for patients: the costs and consequences. Br J Gen Pract. 2016; 66(644): 145.
- Maher L, Gustasfson D, Evans A. Sustainability model and guide. 2015. Available at https://www.dur.ac.uk/resources/public.health/middlesbrough/event/7.2.1. NHS Sustainability Model February 2010.pdf. (Accessed on 31st January 2021)
- Silver SA, Harel Z, McQuillan R, et al. How to Begin a Quality Improvement Project. Clinical Journal of the American Society of Nephrology. 2016; 11: 893-900.
- Blackhouse A, Ogunlayi F. Quality Improvement into practice. BMJ. 2002. https://m865doi:10.1136/bmj.m865
- Royal College Surgeons of Ireland Online Library Repository.
- Khalid MA. Satisfaction of Patients Attending in Primary Healthcare Centers in Riyadh, Saudi Arabia: A Random Cross-Sectional Study. J Relig Health. 2017; 56: 876-883. doi.10.1007/s10943-016-0268-x
- Pryce A, Mccann D. Delayed flow is a risk to patient safety: A mixed method analysis of emergency department patient flow. International Emergency Nursing. 2021.
- Howe W, Geraldi J. Gantt charts revisited: a critical analysis of its roots and implications to the management of projects today. International Journal of Managing Projects in Business. 2012; 5(4): 578-594
- Health Service Executive (2018) People’s Needs Defining Change. Health Services Change Guide. Dublin: Health Service Executive.
- Ortiz-Ospina E, Roser M. Financing Healthcare. 2021. Available at https://www.ourworldindata.org
- Orlewska E, Gulacsi L. Budget-Impact Analyses: A Critical Review of Published Studies. Pharmacoeconomics. 2009; 27(10): 807-827.
- Saha S, Carlsson KS, Gerdtham U, et al. Are Lifestyle Interventions in Primary Care Cost- Effective? – An Analysis Based on a Markov Model, Differences-In-Differences Approach, and the Swedish BjoÌrknaÌs Study. 2013. (Available at: http://www.plusone.org, accessed 12.01.2021)
- Bates DW, Gawande AA. Improving patient safety with information technology. New England Journal of Medicine. 2003, 348: 2526-2534. Available at https://scholar.google.com/scholar?hl=en&as_sdt=0%2C5&q=bates+and+gawande++2003&btnG=#d=gs_qabs&u=%23p%3DATc50toTK7gJ
- Kumar RDC, Khiljee N. Leadership in healthcare. Journal of Anesthesia and Intensive Care medicine. 2015.
\